As a pediatrician, one of my passions is advocating for the health and well-being of children.
Having cared for many children during my ten years in the Navy on active duty and my five years at Canyon View Pediatrics, I’ve realized that often our goal shouldn’t be forcing children to be a certain way but embracing all that they can become. Since moving to South Utah County 5 years ago, I’ve put this philosophy into action by serving on the Board of Directors for Kids Who Count.
Kids Who Count is a non-profit organization serving Nebo SchoolDistrict. The group is dedicated to bringing minimal to no cost early intervention services to children 0 to 3 years old who have delays in speaking, walking, or social development. Over the last year, following many years of planning and organization, I’ve also been able to bring Autism treatment services to the area, allowing families to find help closer to home instead of traveling to Provo, Lehi, or even further.
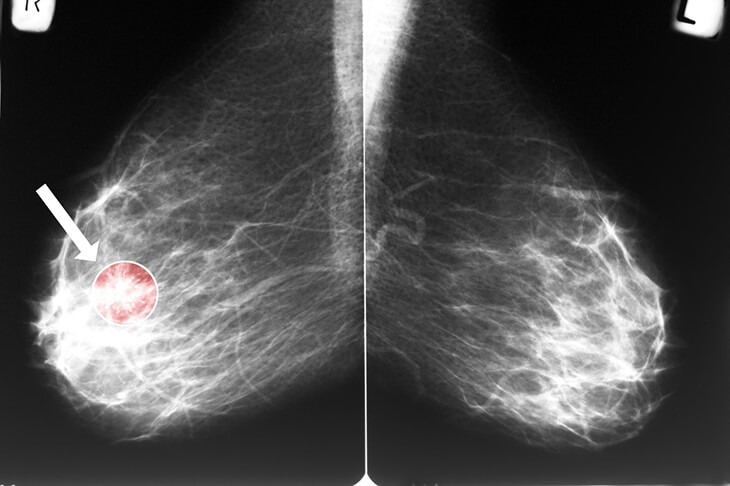
October is breast cancer awareness month. It’s a great time to go over a few common questions women have regarding breast health and breast cancer detection.
The first step in breast health is breast self-awareness, which means that you are aware of what is normal for your breast and can detect small changes. Self-detection results in almost one-half of all cases of breast cancer being found in women aged 50 years and older. A woman herself often finds breast cancer. In women younger than 50 years, more than 70% of breast cancer cases are self-detected.
Are there signs and symptoms related to breast cancer?
The most common symptom of breast cancer is a new lump or mass. A painless, hard mass with irregular edges is more likely to be cancer, but breast cancers can be tender, soft, or round. They can even be painful. For this reason, it’s essential to have any new breast mass, lump, or breast change checked by experienced healthcare professionals.
Other symptoms can include –
Swelling of all or part of a breast (even if no lump is detected).
Skin dimpling (sometimes looking like an orange peel).
Breast or nipple pain.
Nipple retraction (turning inward).
Nipple or breast skin that is red, dry, flaking, or thickened.
Nipple discharge (other than breast milk).
Swollen lymph nodes (sometimes breast cancer can spread to lymph nodes under the arm or around the collar bone and cause a lump or swelling there, even before the original tumor in the breast is large enough to be felt).
Should I have a clinical breast exam?
Yes! A healthcare provider should perform a clinical breast exam and can help find lumps that may need further testing and evaluation. The exam should be done every 1-3 years for women aged 25-39 and women aged 40 and older should have an exam every year.
How do I know I am at an average or higher risk for breast cancer?
A woman is considered at higher risk if there is a family history of breast cancer, ovarian cancer, or other inherited types of cancer; BRCA1 and BRCA2 mutations; chest radiation treatments at a young age; and history of high-risk breast biopsy results. Women without these risk factors are at average risk. If you meet the criteria for higher risk, you should speak with a healthcare professional to develop a plan that may include earlier mammograms and/or genetic testing.
When should I start having mammograms?
The American College of Obstetricians and Gynecology recommends that a woman of average risk start at age 40 and have mammograms every 1-2 years. For more information regarding mammograms, click on the link in the reference section below or speak to your healthcare provider.
Early detection of breast cancer is an essential factor in survival rates. Having yearly wellness exams is a great way to stay on top of your health. We would love to answer any questions you have regarding breast health or any part of your wellbeing.
One of the more common conditions we see in Family Medicine is depression. Depression is the most common mental health condition experienced in the general population. About 15% of the adult population will experience depression at some point in their lifetime.
Symptoms of depression can include feeling low, down, sad, or blue. However, there are many mental as well as physical complaints that can be signs of depression. Other common symptoms may include apathy, disinterest, inability to feel anything, problems with sleep, appetite, concentration, motivation, and social withdrawal.
Most people feel low and sad at times. These feelings are normal reactions to life and are experienced when going through different life stressors such as losing a loved one, getting fired from a job, divorce, and other difficult situations. However, prolonged feelings of sadness, hopelessness, and despair that persist can signify depression.
I often find depression, and symptoms of depression are much more subtle and difficult to spot in oneself and those close to us; thus, symptoms may be missed and treatment not started. Currently, the American Academy of Pediatrics now recommends regular depression screening for all adolescents 12 and over, given that adults often overlook the symptoms of depression. Similar screening recommendations exist for adults.
A tool called PHQ-2 can be an easy and quick screening for depression. This tool consists of two simple questions that one can ask themselves or a loved one. The questions are:
Have you often been bothered by feeling down, depressed, or hopeless during the past two weeks?
Have you often been bothered by having little interest or pleasure in doing things during the past two weeks?
A single “yes” answer of more than half or every day indicates possible significant depression, and one should seek further evaluation and care. Thoughts of death necessitate medical attention, and a plan to self-harm requires emergent care.
The good news is there are many effective treatments if you or a loved one is struggling. Effective treatments for depression may include medications, working closely with mental health professionals, and learning different coping mechanisms. Working closely with one’s healthcare provider is a great starting place to help determine the best course of treatments.
When babies are born, we spend a lot of time loving their beautiful faces, but a lot of their care seems to be for their bottoms! A newborn baby typically has 8 to 12 diaper changes in a day—while a person might know a lot about what happens down there, as a parent of a newborn, you may be surprised by what you find. Hearing about it early may help calm some of those middle-of-the-night panic moments. Here are some common findings, questions, and even surprises that may come up during your baby’s diaper change.
Urinating
How often should your baby pee? Your baby should work up to at least 5 to 6 wet diapers per day. A good rule of thumb is Days of Life = Number of Diapers. So 1st day of life, have 1 wet diaper; 2nd day of life, 2 wet diapers; and so on until he reaches 5-6 wet diapers per day from then on. Decreased wet diapers may be the first sign of dehydration, so if you see that your baby isn’t peeing as much as usual, consider shortening those feeding intervals and feeding her more often. If it is a big or persistent drop, she isn’t acting well, or you have other concerns, seek medical attention right away.
Sometimes, in a baby’s urine, you’ll see an orange tinge or even a little pile of orange dust! This is caused by urate crystals. Urate crystals occur because newborn urine is more concentrated in the first few days of life. If you see these, it will likely be in the first week of life. Sometimes, this is referred to as “brick dust” because it often sits on top of the diaper.
Poop
Ahh, poop. I never thought poop would be so important in my medical or parenting career, but the newborn phase is the new parent’s inauguration into the poop obsession club.
Your newborn’s poop will start out as sticky, black/dark green meconium, which will go away by his 4th day of life. After that, diaper changes will be less sticky and tricky. His poop may then be various shades of green, yellow, or brown. Talk to your pediatrician if your baby’s meconium has not transitioned by the 4th or 5th day of life.
Unlike wet diapers, we worry less about how many dirty diapers each baby has. He may poop with every feeding or just every few days. Pooping might even take a bit of effort, accompanied by a red face and a little cry. (It is hard to bear down and relax at the same time!) But if your little one is otherwise happy and gaining weight appropriately, we will be happy too.
So when will your pediatrician REALLY worry about poop? If it is red or black like new blood or old blood, or chalky white, which means it could be missing bile. If there are tiny drops of blood in your baby’s poop, schedule an appointment with your pediatrician. But if you see lots of blood or white-colored stool in your baby’s diaper, he should be seen by a medical professional immediately.
Is that blood down there??
Occasionally, a parent is put in shock from seeing blood in the front of the diaper. Where does this come from?
In baby girls, blood may come from the vagina. Your little girl is born with functioning reproductive organs, so as her mother’s hormones decrease in her body outside of the womb, it may stimulate a “mini period” in her. It can also cause a little bit of clear, white, or yellow vaginal discharge that has a mucus consistency. But no need to worry if either of these things does not occur—though it can happen, it will not necessarily happen in all baby girls.
A baby boy may have small amounts of blood in his diaper after a circumcision. Otherwise, he should not bleed. Normal bleeding from a circumcision site is spotting, less than the size of a quarter. If you see continued dripping or oozing when you are home, try applying pressure for at least 30 seconds. If it does not stop, he should be seen right away by a doctor. Not sure if it’s blood, or is your baby uncircumcised? Consider the possibility of urate crystals. If you think it could be blood, call your doctor right away.
While the rest of us have a #1 and #2, maybe babies should have a #3, #4, or more! Now that we have reviewed what some of those things are, you can be assured when your baby makes the normal transition from being inside the womb to outside. If you have other questions, consider taking a photo of the diaper to share at your appointment when you come to see your pediatrician at Canyon View Pediatrics. Happy diaper changing!
And remember, if your baby is acting ill, excessively sleepy or fussy, has a temperature of 100.4 F or higher, or if you have any other immediate concerns, you should always take your baby in to be seen right away.
A day trip to Lagoon is a fun-filled adventure! The excited anticipation of the rides – the thrill and fear they bring. The sounds of people enthusiastically talking – both in passing time, waiting in long lines, and the jubilant exchanges after the ride is over. The speed of the coasters, gravity-defying movements, blur of colors, and action everywhere. The smell of burgers and fries, waffle cones, and hot pretzels. The refreshment of a cold drink and Dippin’ Dots. You don’t want the day to end, but as the sun begins to go down, the feeling of satisfaction and fatigue is real and you welcome the call of your comfortable bed.
A season at college for young adults is a life-changing experience! The nervous enthusiasm of starting a new chapter in life – both the dreaming and the dread. New friends and new classes. Confident venturing into unfamiliar buildings and landscapes. Novel self-reliance on finances, cooking, cleaning, and laundry. Adventuring to activities alone, without the familiarity of home and comfort of childhood friends. Being exposed to diverse ideas, people with varied upbringing and value systems, and having expansive dreams of the future. Days and nights are filled with fun, yet demand focus and perseverance. As the distant dream of graduation becomes a reality, the physical and mental exhaustion is real. The time spent in pursuing knowledge, skills, and friendships, however, can last a lifetime and has the potential to change you for the better – forever.
Whether you are dreaming of or dreading heading off to college, preparation will make this adventure more meaningful and fun. Here are some common challenges to consider when transitioning to college life:
Living away from home. College facilitates decision-making skills, independent living, self-reliance, and responsibility. You will be staying in a tight living space with minimal storage. Less is more when it comes to packing. Bring items that can be shared.
Managing your time and new found freedom. In college, it is your responsibility to go to class, do your homework and pass your tests. You will be tempted to stay out too late, eat differently, and party. You will need to figure out how to organize and motivate yourself, balance school, work, sports, social and religious activities. Use technology to get organized and schedule your time wisely. Learn to work your plan and plan your work.
Navigating academic changes. College classes necessitate more reading, writing, and analysis than you may be used to. They typically require more papers, have tougher exams, and rarely give extra credit. Be proactive in the learning process. Meet with your professors, use college-tutoring labs, and find effective ways to study on your own and in groups.
Feeling overwhelmed. At times you will feel overwhelmed. Set high, but realistic expectations for yourself and learn how to deal with stress, and pick yourself up after failing. Avoid substance use as it may lead to abuse and impaired decision-making. Change your habits or attitude when necessary and ask for help when you get stuck. Seek counseling services if you are feeling lonely or having a difficult time adjusting to college life, roommates or stress. If suicide is a concern, call 800-273-8255.
Finding a major. It often takes time to figure out what you want to do with your life. Start with general education courses and work with a school counselor. Academic settings can do personalized testing to help you discover your talents and values which can point you in a career direction. Talking to professionals and job shadowing are beneficial. Remember, nothing is “perfect”. There will be pros and cons to every career.
Avoiding drastic changes in nutrition and physical activity. Without careful attention to diet, many college students put on the dreaded freshman 15… or even more. Many students go from being very involved in sports or physical activities in high school to sitting longer in class, staying up later to study, and eating to stay awake. Physical activity needs to purposely be planned into your new lifestyle. Do not wait until you have time or “feel like it,” because you probably never will.
Use extreme caution with meal plans, eating out, and consuming empty calories (such as alcohol). Quick and easy foods are typically over-processed and loaded with calories. Create habits with nutrition and physical activity that will help you later in life. Remember, this is the only body you ever get.
Learning how to budget. College is different from any kind of learning you have experienced before. You get to pay for the privilege of going to school! Be realistic about your expenses and plan for them. Honestly decide what you need and what things you want. Take a class on basic budgeting or seek guidance from a trustworthy source. Prioritize basic living expenses first groceries, cooking utensils, cleaning supplies, toiletries. Plan for academic requirements – textbooks, school supplies, and classes fees. Entertainment and relaxation are vital to personal balance and fulfillment but do not need to be costly. You are accountable for your finances. Keep records of school expenses for tax purposes.
Avoiding infections or unplanned pregnancy. Abstinence or consistent use of condoms are the only ways to protect against sexually transmitted infections or unwanted pregnancy. Please ask your provider what is the best method for you. Be aware of date rape, increased incidence of sexual assault with substance use, and learn self-defense strategies and techniques to help prevent these conditions.
Make this season of your life a fun-filled adventure! Meet new friends, discover who you are, establish a strong foundation for your future career and become a life-long learner. Talk to a trusted friend, adult, or care provider if you have questions about going to college.
Hormone therapy at the time of menopause and beyond is one of the most controversial subjects in Gynecology. Historically, the replacement of Estrogen and Progesterone was felt to have nothing but benefits. Increased bone health, reduction in hot flashes, and relief from atrophy of the genital tissues are all known benefits. It was once thought that Hormone Therapy (HT) improved heart health since women develop heart disease in general later than men. Lower risk of heart disease has not been proven, and it may increase the risk of certain cardiovascular conditions. There also appears to be a slight increase in the risk of some types of breast cancer in long-term users of HT. So, why would we use HT knowing the risks? In short, it is because menopause can be miserable for some women!
Menopause occurs on average around age 50 and is defined as no periods for at least a year. The transition leading up to menopause and afterward can be a time of great distress for many women. Hot flashes are often more than just a nuisance, and at night, when they manifest as night sweats, they can be very disruptive to sleep. Mood changes are common, and there can be gradual atrophy of genital tissues leading to dryness, irritation, painful intercourse, and urinary problems.
Many women have mild menopausal symptoms and don’t require HT. However, for the women who suffer from more severe symptoms, it can be a lifesaver to use Estrogen, usually along with Progesterone, to alleviate many of these symptoms. Essentially, one must weigh the risks that are small but real against the quality of life issues. Sleep disruption, in particular, can lead to poorer health and quality of life. Low doses of HT can diminish Hot Flashes and night sweats, decreasing distress and improving sleep quality. Oral pills, topical gels, sprays, and patches are all effective. Vaginal estrogen creams can improve symptoms of genital atrophy in women for whom hot flashes are not a problem.
There are pros and cons to HT, and some women should avoid it altogether if they have specific medical issues. For those who do need HT, we usually try for the lowest dose and consider discontinuation after a time. Whether or not to use HT is a joint decision between you and your doctor. Fear of hormones should not deter women from using HT when appropriate. After all, your body was making these same hormones for 40 years before menopause!
Vaccinations for COVID 19 have definitely been the topic of many heated discussions this past year. I hope to provide professional information to help our patient family make the decision whether or not to vaccinate their child against COVID 19.
What vaccines are available?
At the time of writing, the Pfizer-BioNTech COVID-19 vaccine was the only available vaccine with emergency authorization for use from the Food and Drug Administration (FDA) for children ages 12-17 to prevent the spread of COVID-19 in the United States. The Moderna COVID-19 vaccine was recently given emergency authorization for use in children ages 12-17 in the European Union (EU) by the European Medicines Agency and may soon be available in this country. Full FDA approval for these vaccines are still pending.
What are the health risks of not vaccinating my child?
According to the American Academy of Pediatrics (AAP), the percentage of new pediatric cases of COVID-19 has been increasing when compared to new adult cases. In the month of April 2021, approximately 70,000 new pediatric cases were reported weekly in the United States, accounting for 22.4% of all new cases. (1) Since the onset of COVID-19 there have been nearly 4 million US cases of COVID-19 in children, with up to 2% of those resulting in hospitalization. Some conditions requiring hospitalization were acute respiratory failure, shock, cardiac dysfunction, and Multisystem Inflammatory Syndrome in Children (MIS-C). Although a rare condition, MIS-C has been linked to COVID Long hauler symptoms such as shortness of breath, fatigue, and muscle pain that can persist for many months after recovery from COVID-19. Pediatric Intensive Care Unit admissions were more likely with preexisting conditions such as asthma, prematurity, diabetes, and obesity. (2) Death from COVID-19 has occurred in less than one percent of reported pediatric cases with the majority having preexisting conditions such as previously mentioned. (3) Post COVID associated infection cases of myocarditis (inflammation of heart tissue) in adolescents are also on the rise. (4) It is speculated that the overall rise in COVID cases can be attributed to the different variants that have arisen recently.
What are the risks if my child gets the vaccine?
Side effects have been similar in children 12 – 17 as they are for those 18 and over. Some of the more common side effects of the Pfizer-BioNTech COVID-19 vaccine are pain, redness, and swelling at the site of injection. Other side effects such as fevers, chills, muscle pain, headache, joint pain, and nausea can occur and typically last for one to three days. (5) In certain instances, more serious complications can arise including myocarditis, which has been recognized as a rare complication of COVID-19 mRNA vaccinations, especially for young adult and adolescent males. According to the US Centers for Disease Control and Prevention, when monitoring the vaccinations in June of this year, myocarditis rates after the second dose of COVID vaccination were above what was expected. (6) This prompted an emergency meeting of the CDC’s Advisory Committee on Immunization Practices later that month. During that meeting, the health risks from the vaccine and the health risks of COVID 19 infection were discussed and it was concluded that the benefits from vaccination outweigh its associated risks.
How do I report a reaction to the vaccine?
Vaccine adverse reactions are reported to the Vaccine Adverse Event Reporting System. To report vaccine side effects go to this website: https://vaers.hhs.gov/
Who should not get the vaccination?
Anyone who has an allergy to any of the components of the vaccination should not get it.
The FDA recently made the recommendation for those who have compromised immune systems to have a third dose of the vaccination. This includes children.
What are the recommendations?
It is recommended by nearly every professional medical association in the United States (and worldwide) that all individuals, ages 12 and over, should receive the COVID 19 vaccine, as long as they do not have a specific contraindication. Some of the prominent organizations include the American Academy of Pediatrics, the American Academy of Family Physicians, the American Medical Association, and the American Diabetes Association.
Canyon View Medical Group recognizes that the decision to vaccinate your child against COVID 19 can be difficult with all of the different information available to you. If you have specific questions or concerns, we urge you to please have a discussion with your provider.
(2) Kim L, Whitaker M, O’Halloran A, et al. Hospitalization Rates and Characteristics of Children Aged <18 Years Hospitalized with Laboratory-Confirmed COVID-19: COVID-NET, 14 States, March 1–July 25, 2020. MMWR Morb Mortal Wkly Rep 2020; 69:1081–1088.
(3) Shekerdemian LS, Mahmood NR, Wolfe KK, et al. Characteristics and Outcomes of Children with Coronavirus Disease 2019 (COVID-19) Infection Admitted to US and Canadian Pediatric Intensive Care Units. JAMA Pediatr 2020; 174:868–873.
(4) Lara D, Young T, Del Toro K, Chan V, Ianiro C, Hunt K, Kleinmahon J. Acute Fulminant Myocarditis in a Pediatric Patient With COVID-19 Infection. Pediatrics. 2020 Aug;146(2):e20201509. doi: 10.1542/peds.2020-1509.
Menstruation is part of the average woman’s life for about forty years – from early adolescence until menopause. That’s a lot of periods! While menstruation is a normal bodily function, dealing with the routine of your period can be a pain sometimes. It can be even harder when something is wrong with your period. Whether your periods are too heavy, too crampy, too unpredictable, or just seem off, it is a good idea to get checked out by your healthcare provider. It can feel awkward to talk about something as personal as your period, but please don’t worry – it’s our job to help with all aspects of your health. There are a lot of reasons abnormal menstruation can occur. The good news is that there are treatments that can help with abnormal periods. Here are five common reasons something could be off with your period:
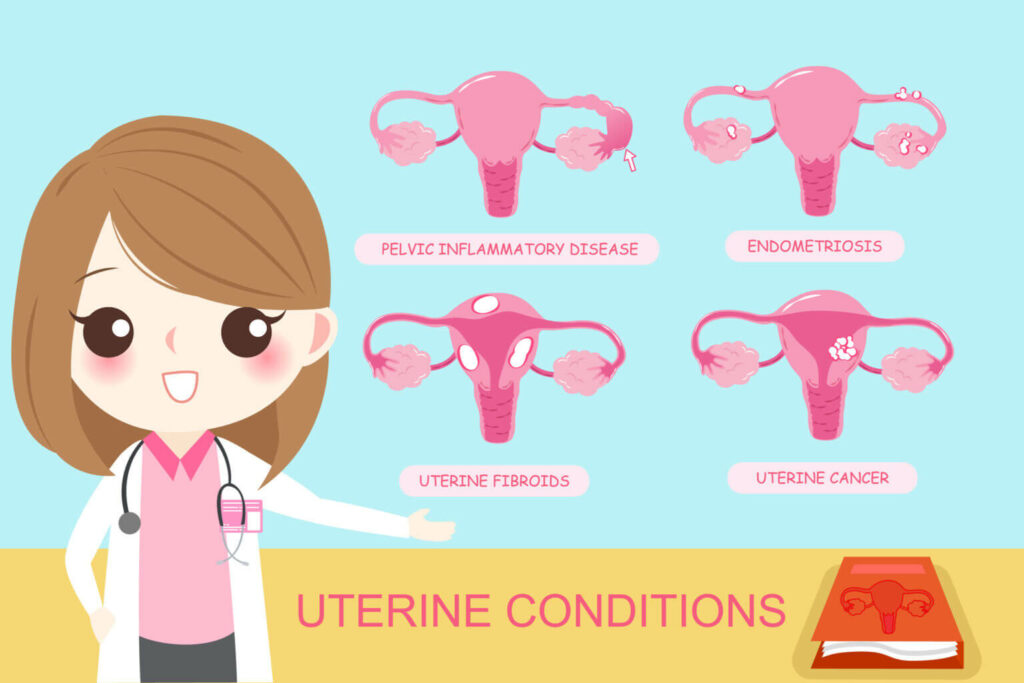
Problems with the uterus.
Sometimes, there is an anatomical or structural cause of abnormal bleeding. These can include different types of benign growths inside the uterus, including endometrial polyps and uterine fibroids. You can also have polyps of the cervix. These things might be diagnosed with an exam or imaging. There are also diseases such as adenomyosis, which involves inappropriate growth of glands into the muscle of the uterus, and endometriosis, which is when small pieces of uterine lining implant outside of the uterus.
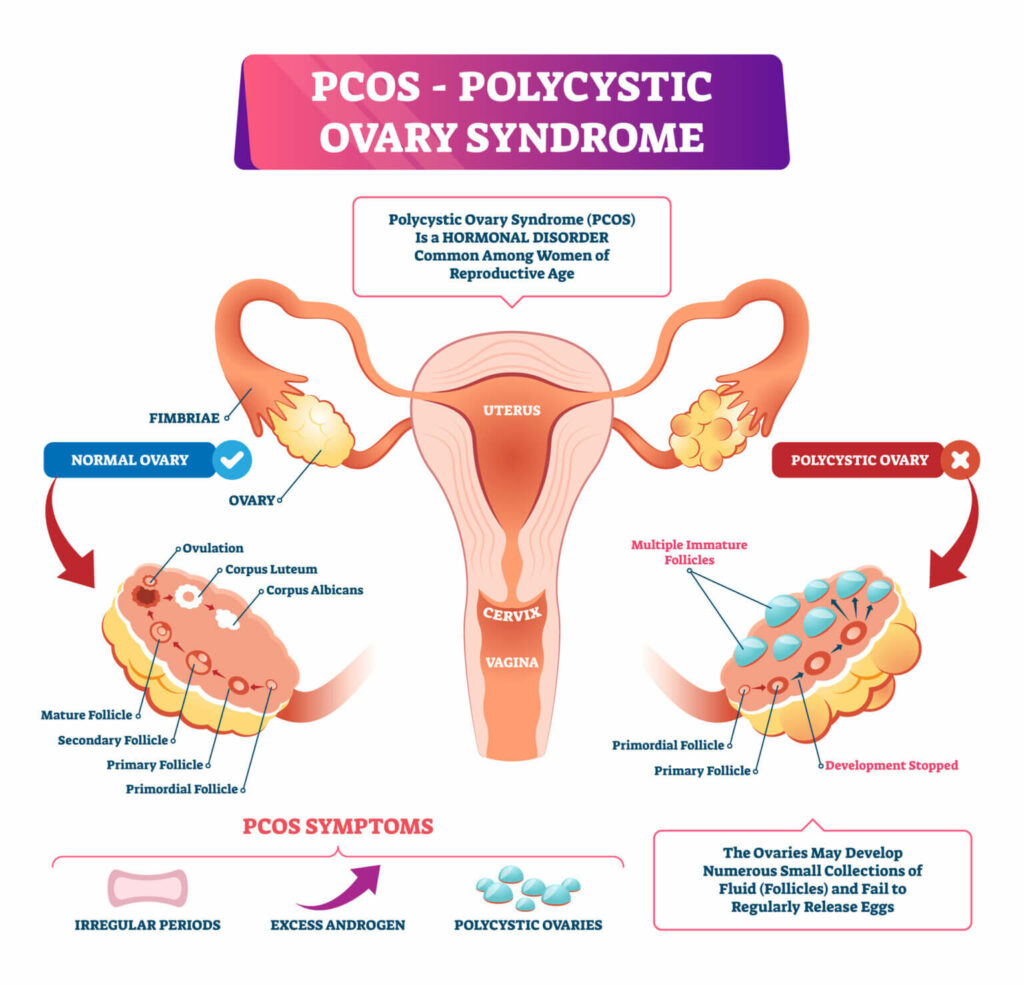
Problems with ovulation.
Normally, you should ovulate, or release an egg, about halfway through your cycle every month. If you are not ovulating regularly, this can cause problems with your period in addition to making it harder to get pregnant. Polycystic ovarian syndrome (PCOS) is a common disease that falls into this category. Thyroid disorders and other hormonal problems can also interfere with ovulation. It is also possible for the timing and regularity of ovulation to be affected by age, weight, exercise, and other factors.
Bleeding disorders.
If you have abnormal periods, it is important to let your healthcare provider know if you have a known family history of bleeding disorders. You should also watch for other types of abnormal bleeding. For example, do you get frequent nosebleeds? Have you been told you bleed excessively after a surgery or dental procedure? Did you experience postpartum hemorrhage with the delivery of a baby? There are many clues that can point towards a bleeding disorder. The most common inherited (genetic) bleeding disorder is Von Willebrand Disease, which affects about 1% of the population. Many other bleeding disorders exist, so talk to your healthcare provider if you have a concern.
Cancer and abnormal cell growth.
While we always hope that cancer is low on the risk of possibilities when something is wrong with our health, it is important to know that uterine cancer can be a cause of abnormal bleeding. Most cancers of the uterus come from the lining, called the endometrium. Endometrial cancer becomes more common with increasing age, excess weight, or long episodes of irregular bleeding Any vaginal bleeding after menopause needs to be evaluated by your healthcare provider. In addition, your healthcare provider can decide if abnormal or heavy bleeding could be a sign of noncancerous abnormal growth of the endometrium, which is called endometrial hyperplasia.
Medications.
With some types of birth control, changes to your menstruation are common and expected side effects. For example, heavier bleeding is a known side effect of the non-hormonal intrauterine device (IUD), while the hormone-containing IUDs may make bleeding lighter. Your bleeding schedule may also change with some types of hormonal birth control. You should also know that certain medications can affect your menstruation. These include anticoagulants and some psychiatric medications. If you have questions about your medications and your bleeding, talk to your healthcare provider.
As you can see, there are a lot of things that can affect your period! This list is by no means comprehensive, and each topic mentioned above could have an entire textbook written about it. If you have any concerns about your menstruation and your health, please don’t hesitate to have a conversation with your healthcare provider. If you aren’t sure what is considered “abnormal” with periods, ask! Some women live with difficult periods when they do not have to, and we may be able to identify the cause of the problem. The proper evaluation and treatment of period problems is so important to a woman’s quality of life. As an OB/GYN Physician Assistant, I am especially passionate about helping women with their menstrual and reproductive health. It is such an important aspect of our lives that is sometimes overlooked. We are always happy to listen to your concerns, answer your questions, and help you manage your health.
If you have questions or concerns about menstrual bleeding please contact our office at 801-465-2559
If you attend yearly wellness evaluations with your regular health care provider, you have probably heard us talk about when you are due for a colonoscopy. So what is a colonoscopy, and why are we talking about it?
A colonoscopy is one of several tests used to identify precancerous changes, early cancerous lesions, or cancer of the colon.
We call cancers of the colon “Colorectal Cancer.” Colorectal cancer is the second leading cause of cancer death for both men and women (preceded only by lung cancer). 52,980 people in the US are expected to die of colorectal cancer in 2021. It is most frequently diagnosed in persons age 65-74. However, 10.5% of new colorectal cancer cases occur in persons younger than 50 years old, and cases of this cancer have increased almost 15% from 2000-2002 to 2014-2016 in persons age 40-49. Because of this change, the US Preventative Task Force recently changed its recommendation for screening colonoscopies to begin at age 45. However, most insurance guidelines still follow the previous guidance of age 50, so this test isn’t covered as a screening test before age 50 yet. (This is different if you have a family history! For example, suppose someone in your immediate family, like a parent or sibling, had colon cancer. In that case, it is recommended you have a colonoscopy when you are ten years younger than your family member was when they were diagnosed, or age 50, whichever comes first.)
Colon cancer often has no symptoms early on when it is easiest to treat. When it does cause symptoms, it can cause stomach pain, a change in bowel movements, blood in bowel movements, and feeling tired or weak. The goal is to find precancerous changes before they progress and cause any symptoms or damage.
So what makes a colonoscopy such a great cancer-reducing tool?
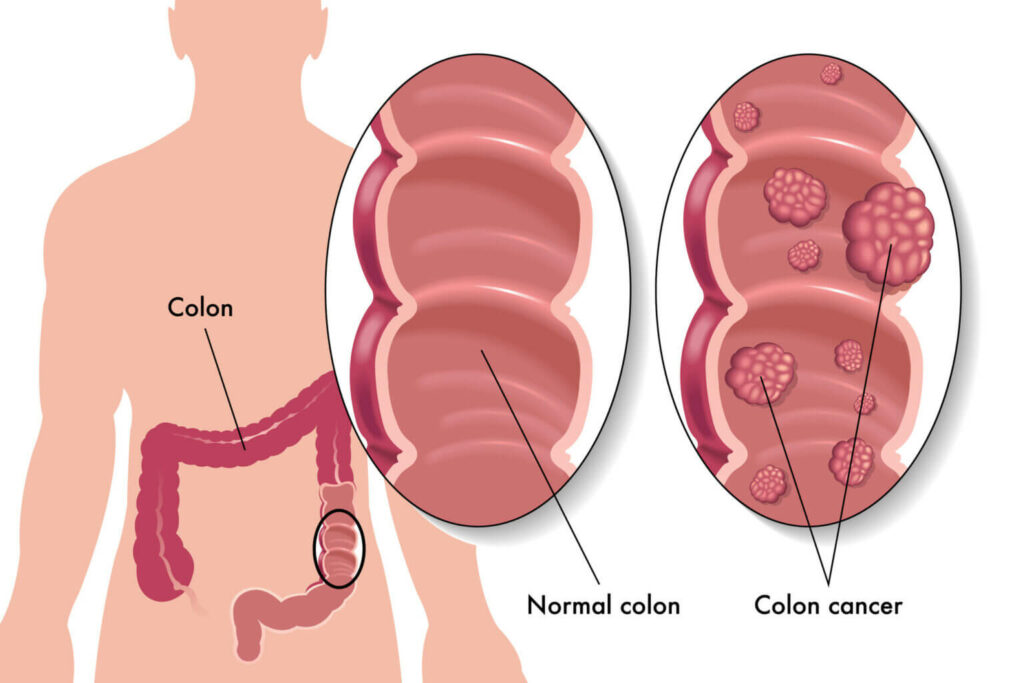
The primary goal of colorectal cancer screening is to prevent deaths from colorectal cancer. Screening tests can help identify cancers at an early and potentially curable stage. Screening can also prevent cancer by identifying and treating abnormal precancerous growths (polyps) that can be removed before they become cancer. So you can be screened and treated for pre-colon cancer lesions, all during the same test.
The Background:
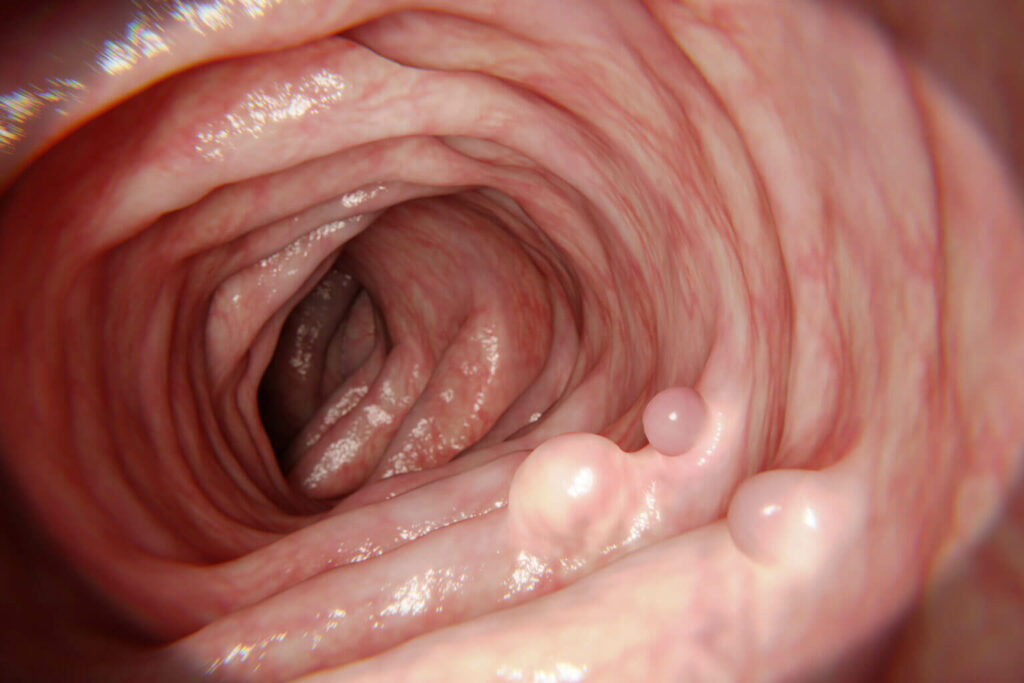
Most colorectal cancers develop from precancerous polyps. Polyps are growths that form in the lining of the colon. These polyps can develop into cancer over time, but this progression takes at least ten years in most people.
So during a colonoscopy, if a polyp is found, it is removed to try to prevent it from becoming more serious. Regular screening with colonoscopies for and removing polyps reduces your risk of developing colorectal cancer by up to 90%! Similarly, if a cancer is found, it may be treated, hopefully at an earlier stage than it would have been found otherwise. Early detection of cancers already presents in the colon increases the chance of successful treatment and decreases the chance of dying due to cancer.
So how do we get ready for a colonoscopy, and how does it work?
The Prep:
Colonoscopy requires that you prepare by cleaning out your entire colon so the provider can see the inside of your colon well. Essentially, they are looking through a small camera to look for changes in the intestine wall lining. So the colon wall needs to be clean for them to see.
This clean-out usually involves drinking a laxative liquid preparation that causes temporary diarrhea. This is by far the worst part of the colonoscopy experience. It is also a reason that many people avoid having a colonoscopy. Avoiding a colonoscopy, for this reason, is foolish as progressive colon cancer will cause far more symptoms than “temporary diarrhea.”
The Procedure:
Once prepped, you will go to your scheduled appointment at the “Colonoscopy Center” we sometimes refer to as the “GI Lab,” short for Gastroenterology Lab. There you will be given a mild sedative drug, or some providers use a more potent anesthetic agent that puts you to sleep. This might be the best part of the colonoscopy, the short but powerful “colonoscopy nap.”
Once you are sedated, a thin, flexible, lighted tube is inserted through the anus and used to directly inspect the lining of the rectum and the entire colon. Biopsies (samples of tissue) may be taken during the procedure. Polyps and some cancers can be removed during this procedure. The whole process usually takes less than 30 minutes. You are given the news of your colonoscopy immediately, but you will need to wait for the pathology results for several days if you had removed polyps during the procedure. Pathology results help determine if additional treatments are required and how many years you can wait before your next colonoscopy.
You can rest and recover from the sedation and must have someone to drive you home and stay with you for several hours as you fully recover from the sedation. After that, you can typically resume life as usual.
Isn’t there an easier way?
There are several other screening tests we use to look for signs of colon cancer. However, none of them are as effective as a colonoscopy. Colonoscopy is the most sensitive of the available tests; it detects most small polyps and almost all large polyps and cancers and substantially lowers the risk of developing and dying from colorectal cancer.
Do we ever use colonoscopies for other reasons?
Yes! We use these useful diagnostic tools to identify other health problems also. For example, blood in your bowel movements, changes in your bowel habits, to evaluate for causes of anemia, or long term belly or rectal pain that we can not explain another way.
So, be as aggressive with your colon cancer screenings as you can! It is an almost entirely preventable cancer if we use colonoscopies effectively! Talk with your provider at your next visit about planning to have this vital screening completed.
I am possibly the best and worst person to write about this topic. Since turning 40 I have broken my collarbone AND my back mountain biking, broken my tibia skiing, torn the cartilage in my knee on vacation last year, and recently injured my hamstring so badly I begged ski patrol to take me down the mountain in the “Sled of Shame”.
I am an uncoordinated, overweight, 53-year-old weekend warrior. But I am trying to be active, trying to eat right, trying to lose weight, and trying to get outdoors.
In the last 13 years, I have backpacked all over Utah, slept on rocks everywhere from the Escalante drainage to the high Uinta mountains, canoed down the Colorado, and biked over 100 miles on the White Rim trail in Canyonlands National Park.
I have thought a lot recently about what I want to be doing when I am 63, 73, and 83, and how I achieve those goals.
I have learned the hard way that physical activity is good, but “catching air”, and setting speed records is bad.
Obviously, that is an oversimplification.
How can we stay active, have fun, and still stay safe?
PROPER CONDITIONING
Preventing injuries starts with proper conditioning. In addition to regular aerobic training, working on strength training and flexibility is key to preventing future injuries. Mixing it up helps; cross-training, or participating in a variety of activities, helps keep you out of the ER or my office. When I stretch and do those boring exercises, I end up staying upright and away from surgeons.
WARMING UP
Warming up before hitting it hard helps. It does take a few more minutes, but that time can save months of rehab after surgery.
THE RIGHT GEAR
Wearing the correct gear is essential. I have learned the hard way that helmets, gloves, elbow, and knee pads are just as important as my bike when I ride trails. Borrowing someone else’s poorly fitting gear can lead to disaster.
Sunscreen and SPF protective hats and clothing are also “the right gear.” Sunburn not only ruins your vacation but can lead to melanoma that can be deadly.
KNOW WHAT YOU ARE DOING
Learn proper technique, know correct form, know and obey the rules. Taking a few classes is never a bad idea, and is often money well spent.
FEED AND WATER YOURSELF
Hydration is extremely important, particularly as June turns to July and August. Make sure you have enough fuel; if you are exercising for long periods of time make sure your body’s fuel tank is full.
DO WHAT I SAY, NOT WHAT I HAVE DONE….
Avoid playing while tired or in pain. Most of my injuries have been on the “last run” or trying to get in “one more mile.” When you are tired, your muscles are just not reliable.
Avoid trying extreme, YouTube-worthy activities or stunts. I see too many injuries in patients of all ages who were trying to copy something they saw on the internet.
If you have questions about how to stay safe, talk to your provider. We can give you information and arrange for referrals to physical therapists and nutritionists who can help you get ready for a lifetime of safe activity!
80 year-olds ski free at Alta, and my personal goal is to get that free season pass in 2047. See you on the lift or on the trails!